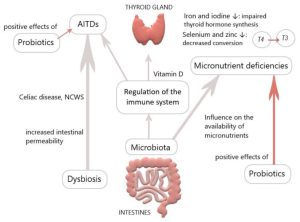
The gut microbiota plays a pivotal role in thyroid disorders, including Hashimoto thyroiditis, Graves’ disease and thyroid cancer. Recent data have suggested that microbes influence thyroid hormone levels through the regulation of iodine uptake, degradation, and enterohepatic cycling.
Studies have been shown that Lactobacillaceae and Bifidobacteriaceae are often reduced in hypothyroidism and hyperthyroidism. In Graves’ disease patients, the composition of the gut microbiota differs from that of healthy individuals, with a significant decrease in the relative abundance of Faecalibacterium prausnitzii, Butyricimonas faecalis, Bifidobacterium adolescentis and Akkermansia muciniphila compared to the control. Furthermore, a diagnostic model was developed using metagenome-assembled genomes of the gut microbiome, which may serve as a valuable predictor for Graves’ disease. The gut microbiota has the capacity to produce various neurotransmitters, such as dopamine, which can regulate the hypothalamus-pituitary axis and inhibit thyroid-stimulating hormone (TSH).
The Effects of Probiotics and prebiotics on thyroid function
Numerous studies have been conducted to investigate the modulation of gut microbiota in order to restore dysbiosis in patients with thyroid disorders. Probiotics and prebiotics have demonstrated beneficial effects on thyroid diseases. Probiotics including bifidobacterium longum supplied with methimazole was implemented in nine patients with Graves’ disease for six months. The results showed a significant reduction in clinical thyroid indexes, including free T3, free T4, and thyrotropin receptor antibody (TRAb), while TSH levels increased compared to baseline. Another study explored the effects of a four-week treatment with a complex probiotics preparation consisting of Bifidobacterium infantis, Lactobacillus acidophilus, Enterococcus faecalis and Bacillus cereus in patients post-thyroid hormone withdrawal (THW) following thyroid cancer surgery. The treatment led to a decreased occurrence of complications such as dyslipidemia and constipation. However, the serum levels of free T4, free T3 and TSH showed no change between groups. Synbiotics, which are a mixture of probiotics and prebiotics, have also been examined. They have shown potential in reducing TSH and increasing freeT3 in patients with hypothyroidism. A strategy based on microbiome-directed therapies, involving supplementation with probiotics, prebiotics and synbiotics holds promise as a therapeutic approach for thyroid disorders.
Conclusion
There is a growing interest in investigating the potential role of probiotics or prebiotics supplementation to improve thyroid function in humans. A recent meta-analysis indicates that supplementation with probiotics/prebiotics has no significant effect on thyroid hormone levels, while showing a modest decrease in TRAb levels. However, the results have been inconsistent, and the probiotics or prebiotics are various in each randomized clinical trial, leading a mixed effect.
بی اشتهایی عصبی یک اختلال رایج خوردن در زنان نوجوان است که درمان موفقیت آمیزی ندارد. مطالعات انسانی و حیوانی اخیر، پیوندهای جدیدی را بین تغییر میکروبیوتای روده، اشتها و تنظیم وزن بدن در بیاشتهایی عصبی نشان داده است.
بی اشتهایی عصبی یک اختلال روانپزشکی بوده که با سوءتغذیه شدید مزمن و گرسنگی مشخص می شود. در اکثر موارد این بیماری در آغاز نوجوانی شروع و کم کم به یک بیماری پایدار تبدیل می شود که در ۴۰ درصد موارد می تواند کشنده باشد. اگرچه درمان بی اشتهایی ترکیبی از گفتار درمانی با تغذیه مجدد است، نتایج نشان داده است که این روش اثربخشی محدودی در بازگرداندن تعادل جسمی و روانی دارد. مطالعات محدودی پیرامون اهمیت ارتباط روده و مغز و تغییرات میکروبیوم روده در ایجاد بی اشتهایی وجود دارد. با این حال، تعیین نقش دقیق میکروبیوتای روده در بی اشتهایی کلیدی برای مداخلات بالینی است.
نقش میکروارگانیسم ها در بی اشتهایی عصبی
دانشمندان دریافتند که در مقایسه با زنان سالم با وزن مناسب، تفاوت هایی در سطوح هر دو جمعیت ویروسی و باکتریایی نمونه مدفوع زنان مبتلا به بی اشتهایی وجود دارد و با افزایش غلظت و تنوع ویروسی، تنوع کلی باکتری کاهش می یابد. با تجزیه و تحلیل ترکیب باکتری های روده هر فرد، متوجه شدند که در زنان مبتلا به بی اشتهایی، سطوح برخی باکتری های مشخص بالا و سطح برخی کاهش داشته و عملکرد آنها نیز تغییر کرده است. به عنوان مثال، کاهش باکتری تولید کننده ویتامین B1 ممکن است کاهش این ویتامین را در بیماران بی اشتهایی عصبی توضیح دهد.
۳۵ متابولیت سرمی مربوط به میکروبیوتا در آزمایش خون این بیماران نیز یافته شده است که با بی اشتهایی در ارتباط هستند، مانند افزایش سطح اسیدهای صفراوی ثانویه و متابولیت های تریپتوفان که در تنظیم سیری و فعالیت سروتونین نقش دارند. این عناصر ممکن است منشأ عدم حساسیت به گرسنگی بوده و در نتیجه به حفظ بی اشتهایی عصبی کمک کنند. با توجه به این موضوع، علائم اختلال خوردن از طریق پرسشنامه ای توسط بیماران تکمیل شد که نشان داد بین فراوانی باکتری های خاص و اعتماد به نفس پایین، کمالگرایی و عدم تعادل عاطفی ارتباط وجود دارد. علائم خاص مرتبط با بی اشتهایی عصبی، مانند تمایل شدید لاغری و نارضایتی از بدن نیز با میکروبیوم روده ارتباط دارند.
دانشمندان همچنین تأثیر میکروبیوتا بر علائم بی اشتهایی را از طریق پیوند نمونههای مدفوع (FMT) از شرکتکنندگان مبتلا به بیاشتهایی و شرکت کنندگان با وزن سالم به موشهای فاقد میکروبهای رودهای مقلد بی اشتهایی با رژیم غذایی محدود سنجیدند. نتایج نشان داد که موشهای دریافت کننده میکروبیوم افراد بیاشتها در ابتدا وزن بیشتری از دست داده و در طول زمان کاهش وزن کمتری داشتند. نتایج این مطالعه همچنین نشان داد که در موشهایی که میکروبیوم افراد بیاشتها را دریافت کردند، بیان برخی از ژنهای سرکوبکننده اشتها (برای مثال، ژنهای Bdnf و Cartpt) در مرکز کنترل اشتهای مغز (هیپوتالاموس) افزایش یافت. در سطح بافت چربی نیز ژنهایی که چربی سفید (ذخیره انرژی) را به چربی قهوهای (مبدل انرژی به گرمای بدن) تبدیل میکنند افزایش یافتند. این نتایج نقش بالقوه تغییرات میکروبیوم روده را در بهبود بی اشتهایی برجسته می کند. با این حال، این روابط علت و معلولی مستلزم بررسی های دقیق هستند.
نتیجه گیری
اگرچه ترکیبی از درمانهای تغذیهای و روانپزشکی باید در هسته اصلی درمان بی اشتهایی باشد اما تجزیه و تحلیل بیشتر لازم است تا با روش هایی از قبیل از بین بردن میکروب های تغییریافته با آنتی بیوتیک ها یا استفاده از FMT یا پروبیوتیک برای القای میکروب های مفید، نقش میکروبیوم روده در بهبودی بی اشتهایی را بسنجد. با اینکه بازگشت وزن نقش اصلی را در توانبخشی تغذیه ای در افراد مبتلا به بی اشتهایی عصبی دارد، با توجه به یافته های فعلی، میکروبیوم روده نیز باید به عنوان بخشی از مداخلات بالینی تغذیه برای درمان بهینه بی اشتهایی در نظر گرفته شود.
مترجم: فاطمه زری میدانی (Fatemeh Zari Meidani)
ویراستار: مرضیه رحیم خراسانی (Marzieh Rahim khorasani)
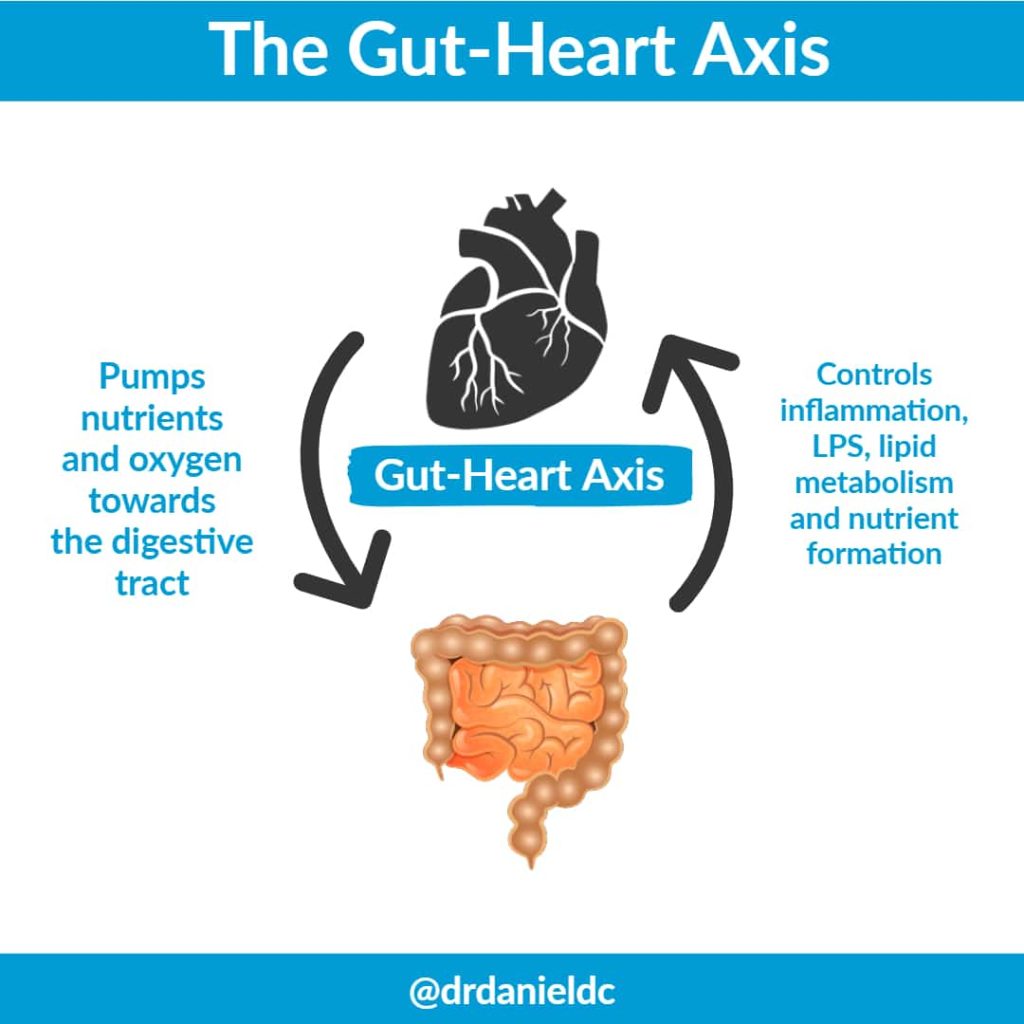
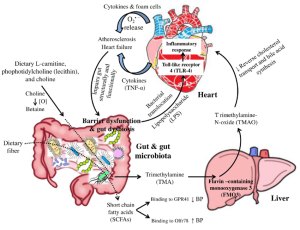
The human intestinal flora is closely related to human health. Gut microbiota dysbiosis is involved in the occurrence and development of various diseases, including coronary heart disease, hypertension, diabetes, inflammatory bowel diseases, and a wide range of inflammatory, metabolic, and neurological disorders. Studies in the last decade have proved that gut microbiota dysbiosis plays a crucial part in host inflammation and the formation of atherosclerosis and hypertension.
Challenges and future perspectives
It is difficult to apply what is known about microbiome composition and function in therapeutic settings. The dynamic nature of the microbiome, particularly it changes throughout illness development and in response to numerous variables such as nutrition, lifestyle, and pharmaceutical therapies, must be understood in order to address this, which calls for longitudinal investigations. Deeper research projects employing cutting-edge approaches like next-generation sequencing, metatranscriptomics, metaproteomics, and metabolomics, as well as computational methodologies, are currently of the utmost importance.۴ We can now investigate the complex interactions of the Heart–Gut axis thanks to these instruments. We will be able to identify the processes by which the gut microbiota affects medication metabolism and response by merging functional analysis, simultaneous profiling of the gut microbiome, metabolomics, and other omics data. These multifaceted techniques have a great deal of promise for unravelling the complex mechanisms by which the gut microbiota interacts with the host, ultimately revealing insightful information for enhancing medication, therapy and enhancing patient outcomes.
Targeting gut microbiota as a therapeutic option
There is interest in employing microbiome-based therapeutics as a possible therapeutic option for CVDs given the potential impact of the gut microbiota on cardiovascular health. Probiotics, which are living bacteria that provide health advantages when taken in sufficient quantities, are one strategy. Numerous beneficial bacterial strains like bifidum, L. casei, L. Acidophilus, L. zisttakhmir, L. reuteri, L.fermentum, C. butyricum, B.breve,have been tested for the treatment of CVDs both in animal models and humans.
Prebiotics and CVDs study is still in its infancy, but there is mounting evidence that they may have beneficial effects on several risk factors for cardiovascular disease like-blood pressure, cholesterol management, chronic inflammation, oxidative stress, glucose metabolism, and weight management. However, further studies are required to evaluate the effectiveness of these probiotics and the best dosage.
Another method is fecal microbiota transplantation (FMT), which involves inserting healthy donor’s feces into the recipient’s gut. Although research is still being done to determine FMT’s potential therapeutic function in CVDs, it has historically been utilized largely to treat illnesses like Clostridium difficile Following FMT, preliminary research in animal models has demonstrated encouraging improvements in cardiovascular parameters and atherosclerotic reduction. The use of gut microbiota-based therapeutics for CVDs is still in its infancy, and more study is required to completely comprehend the intricate relationships between the gut and the heart and to assess the efficacy and safety of these strategies. Individual differences in gut microbial makeup and responsiveness to therapies may also provide challenges in developing personalized therapy modules and regimen.
Research has shown AST-120, an oral charcoal adsorbent to have beneficial effect in the treatment of CVDs. However, it is unclear how adsorbents may affect the gut microbiota’s composition and its associated metabolites in people with CVDs.
Reference
Majumder S, Kirtikumar RM, Shetty V, Mukherjee S, Narayan P. Cardiovascular diseases and the heart–gut cross talk. Indian Heart Journal. 2023 Dec 7.
مطالعات اخیر نشان می دهد ارتباط عمیقی بین میکروبیوتای روده و بیماری های مختلف، به ویژه سرطان، وجود دارد. میکروبیوتای روده که تعداد بی شماری از باکتری ها، ویروس ها، قارچ ها و سایر میکروارگانیسم ها را در بر می گیرد، از طریق مکانیسم های مختلف نقشی اساسی در حفظ سلامت میزبان ایفا می کند. میکروبیوتای روده به عنوان یک تنظیم کننده حیاتی عمل می کند و بر پاسخ ایمنی تأثیرگذار است در نتیجه بر توانایی بدن برای شناسایی و از بین بردن سلول های سرطانی موثر می باشد. تحقیقات نشان می دهد که تغییرات در ترکیب محیط میکروبی روده میتواند باعث ایجاد اختلال در سیستم ایمنی شود و به طور بالقوه در شروع و پیشرفت تومور نقش داشته باشد.
تغییر میکروبیوم روده و سرطان
میکروبیوتای روده به طور فعال در تولید متابولیت و تعدیل در محیط روده شرکت می کند. برخی از باکتری ها متابولیت هایی مانند اسیدهای چرب با زنجیره کوتاه (SCFAs) تولید می کنند که خواص ضد التهابی دارند و به حفظ یکپارچگی سد روده کمک می کنند. برعکس، دیس بیوز، عدم تعادل در ترکیب میکروبی روده، میتواند منجر به تولید متابولیتهای مضر، تحریک التهاب و آسیب سلولی شود و در نتیجه محیطی مناسب برای سرطانزایی ایجاد کند. به عنوان مثال، در سرطان کولورکتال ارتباط قوی با دیس بیوز میکروبی روده نشان داده می شود. مطالعات تغییراتی را در ترکیب میکروبیوتای روده در افراد مبتلا به سرطان کولورکتال شناسایی کردهاند که بر نقش بالقوه گونههای باکتریایی خاص در ترویج یا مهار رشد تومور تاکید میکند.
تاثیر میکروبیوم روده بر سرطان
تحقیقات در حال ظهور تأثیر میکروبیوتای روده را بر اثربخشی درمانهای سرطان روشن کرده است. روش درمانی ایمونوتراپی که سیستم ایمنی را برای مبارزه با سرطان مهار می کند، با میکروبیوتای روده مرتبط است. مطالعات نشان دادهاند که جمعیتهای میکروبی خاص در روده میتوانند بر پاسخ به ایمونوتراپی تأثیر گذار باشند و پتانسیل دستکاری میکروبیوتای روده برای افزایش نتایج درمان را دارند.
اکتشاف نقش میکروبیوتای روده در سرطان، علاقه قابل توجهی را به مداخلات درمانی با هدف قرار دادن میکروبیوم برانگیخته است. رویکردهایی مانند پروبیوتیک ها، پری بیوتیک ها، اصلاح رژیم غذایی، و پیوند میکروبیوتای مدفوع (FMT) به عنوان استراتژی های بالقوه برای تعدیل میکروبیوتای روده و در نتیجه، تأثیر بر توسعه سرطان و نتایج درمان است.
نتیجه گیری
تحقیقات رو به رشد بر اهمیت میکروبیوتای روده در بیولوژی سرطان تأکید میکند. استفاده از این دانش نویدبخش راهبردهای نوآورانه در پیشگیری، درمان سرطان و پزشکی شخصی است. با ادامه تلاشهای تحقیقاتی برای کشف پیچیدگیهای میکروبیوتای روده و پیامدهای آن برای سرطان، به طور فزایندهای آشکار میشود که این جامعه میکروبی پیچیده این پتانسیل را دارد که رویکرد ما در مدیریت سرطان را متحول کند و راه را برای عصر جدیدی در پزشکی دقیق هموار کند.
تصور میشود که اختلالات عملکردی دستگاه گوارش گروهی از اختلالات پیچیده و چند عاملی هستند که پاتوفیزیولوژی مشخصی ندارند. از سوی دیگر، ژنتیک، اختلالات عملکرد روده و مغز، التهاب مخاطی، تغییرات میکروبیوتای روده، تغییرات حرکتی دستگاه گوارش، و عوامل محیطی، مانند رژیم غذایی و استرس ممکن است عوامل کلیدی در ایجاد این بیماری ها باشند. علاوه بر این، باکتری ها، گاستروانتریت تک یاخته ای یا ویروسی و عوامل بیماری زا مانند کمپیلوباکتر ژژونی، شیگلا سونئی، سالمونلا انتریکا، و اشرشیاکلی ممکن است در بروز این اختلالات نقش داشته باشند.
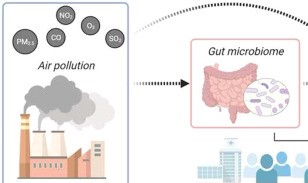
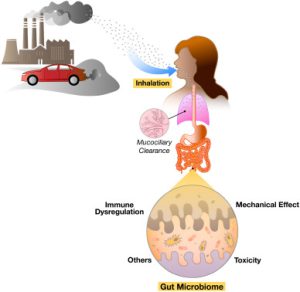
نقش آلودگی هوا در بیماریهای عملکردی گوارشی و میکروبیوم روده
طبق گزارش سازمان بهداشت جهانی، تقریبا ۹۰ درصد مردم جهان در معرض آلودگی هوا هستند. آلاینده های گازی می توانند بردستگاه گوارش از طریق ترویج التهاب سیستمیک تاثیر گذار باشند. از این رو، آلودگی می تواند با تغییرات در تنوع فلور روده باعث دیس بیوز و بیماری های روده ای شود. چندین مطالعه در مورد تاثیر آلودگی هوا برسلامت انسان انجام شده است، به ویژه تأثیر آن بر دستگاه تنفسی و بیماریهای قلبی عروقی با این حال، نقش آلودگی هوا در پاتوژنز بیماری های دستگاه گوارش، مانند اختلالات عملکردی دستگاه گوارش ، هنوز تا حد زیادی ناشناخته است ونیازبه مطالعات بیشتری دارد.
تاثیر آلودگی هوا بر میکروبیوتای روده در سال های اخیر به طور فزاینده ای مورد توجه قرار گرفته است. تاریخچه مطالعات در مورد رابطه بین آلودگی هوا و میکروبیوم روده انسان به سال ۱۹۸۹ برمی گردد. این مطالعه به کشت گونه های باکتریایی مربوط میشد که نشان داد مواجهه شغلی با فلزات سنگین همراه است با افزایش انتروباکتریاسه های مقاوم به جیوه در میکروبیوم روده. علاوه بر این، مطالعات دیگر نشان داده اند که میکروبیوتای روده می تواند ذرات بلعیده شده را به متابولیتهای سمی تبدیل کند در نتیجه، این متابولیت ها به گردش خون آزاد می شوند.
آلاینده های بلعیده شده می توانند یکپارچگی سد روده را به خطر بیندازند و به دلیل تأثیر بر میکروبیوتای روده احتمالاً ترکیب میکروبیوم روده را تغییر می دهند. آلاینده های جذب شده ممکن است فراوانی میکروارگانیسم های مفید مانند لاکتوباسیلوس و بیفیدوباکتریوم که نقش حیاتی در محافظت از روده ایفا می کنند را کاهش دهند. آلاینده ها می توانند فراوانی عوامل پیش التهابی را افزایش دهند. همچنین افزایش گونه های باکتریایی از خانواده Bacteroidaceae با میزان بالای O3 مربوط است. شایان ذکر است که قرار گرفتن در معرض آلودگی هوا ناشی از ترافیک می تواند فراوانی باکتروئیداسه را کاهش داده و فراوانی Coriobacteriaceae را افزایش دهد. در نهایت، آلاینده ها محتلف هوا مانند ازن، SO2 و PM می توانند شمار فاسکولارکتوباکتریوم، اگرتللا و کلستریدیوم را تغییر دهند.
The gut microbiome has been identified as a potential factor in weight regulation. Thirty-nine percent of the adults are overweight (25–۲۹.۹ kg/m2) and 13% are obese (BMI≥۳۰kg/m2) worldwide. Recently, it has been found that obesity may affect brain function and structure, as it is associated with impaired cognition and alterations in gray matter (GM) and white matter (WM). Moreover, a higher BMI and waist-to-hip ratio (WHR) have been associated with lower fractional anisotropy (FA) values. Moreover, it is proposed that obesity increases the risk of developing dementia later in life by 60–۹۰%, versus healthy weight individuals. A growing of evidence reveals that obesity is related with alterations in neuroendocrine production and secretion, including ghrelin, insulin, GLP-1 and PYY.
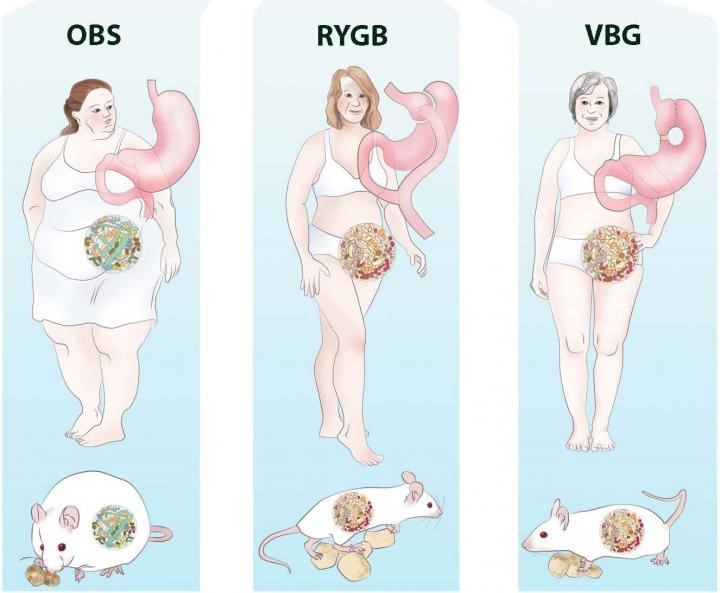
Bariatric surgery for obesity treatment
Bariatric surgery is an effective treatment for obesity leading to rapid and sustainable weight loss. Bariatric surgery decreases body weight not only due to physical effects such as reduced food intake and malabsorption but also due to the various neuroendocrine changes which affect energy homeostasis and hunger/satiety. Moreover, Bariatric surgery might improve the gut microbiota diversity and restore white adipose tissue function, which can improve obesity-related immunological and cognitive impairments. The gut-brain axis consists of a bidirectional communication system, connected through the vague nerve, spinal fibers and sympathetic and parasympathetic fibers which are directly innervating the gastrointestinal tract. These elements communicate through endocrine messengers, neuro-immune mediators and neuroactive metabolites.
Conclusion
To summarize, Bariatric surgery is a good procedure to treat obesity and its related pathologies, however long-term effects remain unsolved. Future research should focus on the long-term effects of Bariatric surgery, to be able to investigate the neuroendocrine, microbiota and white adipose tissue changes and to potentially determine the new “normal” after homeostatic adjustments. Various studies have focused on neuroendocrine alterations already after six months. Six months post-surgery patients lose weight rapidly and generally still follow their post-operative diet. Therefore, the observed effects 6 months post-surgery might differ at longer follow-ups, when patients achieve a stable weight, or regain weight.
The mutual relationships and metabolic activities among microorganisms have a significant impact on modulate hormone levels, especially estrogens in women. The gut microbiota mainly controls estrogen levels through the secretion of β-glucuronidase, which is encoded by several microbiome genera, including Bacteroides, Bifidobacterium, Escherichia, and Lactobacillus. β-glucuronidase enzyme converts conjugated estrogens to deconjugated forms in the gastrointestinal tract. These deconjugated and unbound “active” estrogens enter the bloodstream and subsequently act on estrogen receptor alpha (ERα) and estrogen receptor beta (ERβ), eliciting downstream activation of intracellular signaling cascades, gene transcription, and epigenetic effects. A decrease in β-glucuronidase activity due to an imbalance in the GM community (dysbiosis), there is less estrogen deconjugation, resulting in lower circulating estrogen levels. Conversely, increased β-glucuronidase activity can increase estrogen levels. Thus, maintaining optimal β-glucuronidase activity is critical for regulating estrogen levels in females. Estrogens contribute to epithelial proliferation throughout the female reproductive system and have been shown to drive proliferative diseases such as endometriosis and polycystic ovary syndrome (PCOS).
There is evidence of lower SCFAs concentrations in fecal samples from PCOS patients. Indeed, probiotics’ supplementation promoted the growth of Faecalibacterium prausnitzii, Bifidobacterium, and Akkermansia, which are SCFA-producing bacteria, and can lead to an increase in intestinal SCFAs. In turns, SCFAs bind to their receptors on enter endocrine cells and directly stimulate the release of gut–brain mediators that can influence sex hormone secretion by the pituitary gland and hypothalamus via the gut–brain axis.
Vaginal Microbiota Transplantation and Gynecological Disorders
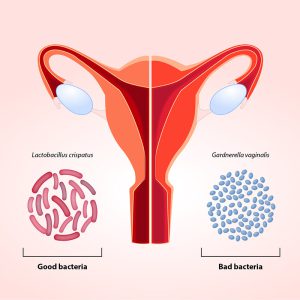
Gynecological disorders that have been explored in relation to Vaginal Microbiota Transplantation (VMT) include bacterial vaginosis, vulvovaginal candidiasis (VVC), and specific cases of infertility. These conditions are often associated with an imbalance in the vaginal microbiota, characterized by a decrease in beneficial Lactobacillus species and an overgrowth of pathogenic bacteria or fungi. The use of microbiota transplantation from healthy women has been suggested as a potential therapy to address imbalances in the vaginal microbiota, known as vaginal dysbiosis. Studies in rat models of vaginal dysbiosis have demonstrated that VMT can be therapeutically effective in reducing inflammation and increasing the presence of Lactobacilli, as well as relieving endometritis-like symptoms (inflammation of the lining of the uterus). The benefits of therapeutic VMT have also been demonstrated in patients with symptomatic, intractable, and recurrent bacterial vaginosis, and this has opened a new avenue for such future studies.
Bacterial vaginosis (BV) refers to a condition in which there is a disturbance in the normal microbial community of the vagina. As well previously documented, usually, the vagina is predominantly inhabited by Lactobacillus species. However, in BV presence, there is a shift in the vaginal microbiome, leading to the emergence of anaerobic bacteria. BV may be associated with a risk of upper genital tract infections, pregnancy complications, and susceptibility to sexually transmitted infections. Currently, there are many limited treatment options in patients with persistent or recurrent BV despite multiple attempts at antibiotic treatment. In addition, probiotic treatment of symptomatic patients with oral and/or vaginal administration of bacterial strains of Lactobacillus has yielded conflicting results, suggesting that the microbiome as a whole, rather than a single bacterial species, may be effective for severe BV.
An experience presentation
Lev-Sagie et al. performed the first exploratory study testing the VMT approach from healthy donors as a therapeutic alternative for patients suffering from symptomatic, intractable, and recurrent bacterial vaginosis (Clinicaltrials.gov NCT02236429). Four out of five VMT recipients experienced a significant improvement in both clinical symptoms and the composition and function of the dysbiotic vaginal microbiome, which persisted over an extended follow-up period, while one recipient experienced partial remission. The authors reported no significant side effects and no serious adverse events. While the lack of adverse outcomes is reassuring, the small study size and lack of a placebo arm make it difficult to interpret whether VMT provided an additional benefit over antibiotics alone. Additional clinical trials are currently ongoing with the goal of further evaluating whether VMT could serve as a viable option in symptomatic and intractable BV
Other Microbiota-Changing Strategies and Future Perspectives
In addition to FM, there are other strategies such as diet, and the administration of prebiotics, probiotics , synbiotics, and postbiotics. Recent research has documented that more than 50% of the diversity in the microbiome can be attributed to food, while host genetics only slightly influence the composition of the microbiota. In detail, a diet high in fiber promotes a significant rise in species producing SCFAs. A high-protein, high-fat, low-fiber diet, on the other hand, is linked to decreased biodiversity and an increase in species that could cause inflammation. A brief food change may cause a change in the gut’s population, but these modifications seem to be temporary. Diet may increase the success of FMT by fostering a favorable environment for the engraftment of donor microbiota and by exerting its own anti-inflammatory effects.
However, these natural approaches lack a direct-targeting action for gut microbiota shaping. For this purpose, researchers have developed the use of engineered bacterial (EB) strains to influence and manipulate the composition and behavior of the microbiota in a promising targeted manner. EB strains can be designed to produce specific metabolites or molecules that, interacting with the microbiota, can influence its composition or activity, showing beneficial effects on human health. EBs are rightly considered the next-generation microbiota therapeutics. In addition, they can be designed to express functions that address monogenic inborn errors of metabolism or to exert a tumor-killing activity.
However, although FMT is a valid therapeutic approach for certain diseases, it shows some procedural limitations. The preparation of fresh or frozen fecal suspensions requires the constant and periodic presence of healthy donors which must be negative in a series of serological and microbiological screening tests. Moreover, the stool samples have to be processed within six hours after collection for preserving anaerobes.
Furthermore, it is essential to know in detail the bacterial composition of the suspension to be infused into the recipient, in order to increase FMT efficacy and especially safety. For these reasons, the therapeutic efficacy of a synthetic bacterial preparation called “Bacterial Consortium” is now under development. This approach involves the isolation from healthy donors’ stool samples of several bacterial species normally present in the human intestinal microbiota, and thus the use of this “Bacterial Consortium”, composed by 13 microbial species, as a safe and valid alternative to donor stools. In conclusion, understanding the mechanisms by which the human microbiota can influence the progression of diseases, including gynecological disorders, can lead to the development of personalized approaches to shape the microbiota composition (and so its function), improving the symptoms and patients’ prognosis.
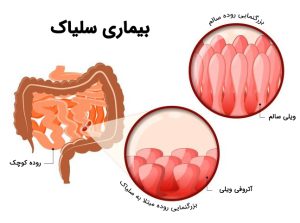
سلیاک یک بیماری شدید خود ایمنی است. در این بیماری، سلولهای ایمنی، روده کوچک را مورد حمله قرار می دهد. سلیاک حساسیت شایعی است که در افرادی با برخی از ژنها هنگامی که گلوتن را مصرف میکنند رخ میدهد. گلوتن در غلاتی مانند گندم، جو و چاودار وجود دارد. این افراد بدنبال مصرف این غذاها دچار سوء جذب و دل درد می شوند. اخیرا ارتباط سلیاک با میکروبیوتای روده کشف شده است. میکروبیوتا، گروهی از میکروارگانیسمها هستند که در روده ما زندگی میکنند و تعادل و تنوع آنها ضامن سلامتی بدن است.
مقایسه میکروبیوتای افراد سالم با بیماران سلیاکی
تحقیقات نشان میدهد ترکیب میکروبیوتا در افراد مبتلا به بیماری سلیاک با افرادی که این بیماری را ندارند، متفاوت است. در واقع، بیماران مبتلا به بیماری سلیاک در مقایسه با افراد سالم دارای کاهش در گونه های مفید و افزایش در گونه های بالقوه بیماری زا هستند. این دیس بیوز ممکن است پس از یک رژیم غذایی بدون گلوتن همچنان باقی بماند. بنابراین، میکروبیوتای روده می تواند نقش مهمی در پاتوژنز بیماری سلیاک ایفا کند. برخی از مطالعات نشان میدهند که ترکیب میکروبها در بدن افراد مبتلا به بیماری سلیاک، به شکلی است که با هضم گلوتن باعث افزایش آسیبپذیری در برابر بیماری می شود. از طرف دیگر، میکروبها در هضم سایر مواد غذایی نیز دخیل هستند و تغییراتی در این فرآیند در افراد مبتلا به بیماری سلیاک مشاهده شده است. به طور کلی، میکروبیوتا میتواند به عنوان یک عامل همراه، بسته به فعالیت و نوع میکروبهای موجود در دستگاه گوارش، منجر به افزایش یا کاهش آسیبپذیری در برابر بیماری سلیاک شود. اما قطعا باید ژنهای مربوطه و تماس با گلوتن نیز وجود داشته باشد.
باید توجه نمود که تبعیت از رژیم غذایی بدون گلوتن در صورتی که بدون نظارت و تجویز متخصص انجام شود، میتواند منجر به کمبود عناصر مغذی و مشکلات دیگر شود. لذا، تشخیص درست بیماری سلیاک و بدنبال آن رژیم غذایی بدون گلوتن از یک طرف و تلاش در جهت اصلاح فلور میکروبی روده از طریق مصرف فیبرها و پروبیوتیکها از طرف دیگر برای مدیریت و بهبود این بیماری بسیار مهم است. به نظر می رسد استفاده از پروبیوتیک ها پاسخ التهابی را کاهش داده و نسبت طبیعی باکتری های مفید را در دستگاه گوارش بازیابی می کند. برای درک بهتر نقش میکروبیوتای روده در پاتوژنز بیماری سلیاک و تأثیر بالینی و استفاده درمانی پروبیوتیک ها در این زمینه، به شواهد بیشتری نیاز است.
افراد بسیاری، در طول زندگی خود، ناراحتی های گوارشی را تجربه می کنند، اما سندروم روده تحریک پذیر (IBS)، اندکی متفاوت است. ازعلائم این بیماری، دل درد، اسهال و یا یبوست می باشد که به طور مکرر رخ می دهد. با این وجود، هیچ نشانی از آسیب به سیستم گوارشی وجود ندارد. بیماران احساس می کنند عمل دفعشان به طور کامل صورت نپذیرفته است. بسیاری از مبتلایان دچار نفخ شده و علاوه بر مشاهده تورم شکم، صداهایی را از شکم خود می شنوند. داشتن درد مزمن و اجابت مزاج های پی در پی، از دیگر مسائل آزاردهنده مبتلایان به این سندروم است.
فوق تخصص گوارش و کبد از مرکز تحقیقات گوارش و کبد دانشگاه علوم پزشکی اصفهان گفت بررسی ها نشان می دهد شیوع IBS در زنان دو برابر مردان است و حدود ۴۰ درصد بیماران به IBS خفیف، ۳۵ درصد به IBS متوسط و ۲۵ درصد به IBS شدید مبتلا هستند. علائم روده تحریک پذیر، اغلب پیش از ۳۵ سالگی بروز پیدا می کند. بسیار نامتعارف است که افراد بالای ۵۰ سال، برای اولین بار، دچار این عارضه بشوند.
بابک تمیزی فرگفت: عوامل مختلفی می توانند در ایجاد سندرم روده تحریک پذیر نقش داشته باشند که برخی از آنها بیشتر از سایرین شایع هستند و می توان با مصرف کپسول colperIBSشرکت زیست تخمیر علائم را کاهش داد.
دلائل عمده سندروم روده تحریک پذیر (IBS)
رشد بیش از حد باکتری های روده کوچک: چنانچه باکتری هایی که معمولا در روده بزرگ یافت می شوند بتوانند در روده کوچک رشد کنند افراد از علائمی مانند درد و کرامپ شکمی مداوم ، نفخ و اسهال گلایه دارند. همچنین رشد بیش از حد میکروارگانیسم های مولد گاز در روده کوچک یا روده بزرگ منجر به یبوست در آن ها می شود.
افزودنی های مواد غذایی: مصرف مواد غذایی فرآوری شده در دهه های اخیر در اکثر کشورها به شدت روند رو به رشدی داشته است. تغییر در محیط میکروبی روده به دلیل استفاده از افزودنی های غذایی می تواند یکی از علل IBS در جوامع باشد. شیرین کننده های مصنوعی نیز می توانند علائم IBS را تشدید کنند. ایجاد IBS با تغییر در میکروبیوم دستگاه گوارش مرتبط است و بنابراین غذاهایی که هضم ضعیفی دارند موجب اختلالات گوارشی بیشتری می شوند.
استرس: در افراد مبتلا به IBS، استرس می تواند آغازگر علائم و یا باعث پیشرفت علائم باشد، بنابراین بسیار مهم است که این افراد همیشه بر استرس خود کنترل داشته باشند. شاید صحبت کردن با یک مشاور، به منظور آموختن راه هایی جهت کنترل استرس، راه حل خوبی برای ایشان باشد.
او ادامه داد، عصاره نعنا فلفلی موجود در کپسول colperIBS شرکت زیست تخمیر با اثر مستقیم روی عضلات روده باعث ریلکس شدن این عضلات میشود. اما به دلیل اثر بر روی عضله ابتدایی معده باعث رفلاکس میشود. استفاده از کپسول انتریک کوت راه حل مناسبی برای جلوگیری از ایجاد اثر بر معده است؛ چرا که با این روش، میتوان از اثرگذاری آن در روده بهرهمند شد و برای رفع دردهای شکمی و تسکین مشکلات شکمی، این ترکیب را به عضلات رودهی افراد مبتلا به سندروم روده تحریک پذیر رساند.
بایدها و نبایدهای غذایی در بیماریهای التهابی روده (IBD) یکی از سوالات اصلی بیماران پس از تشخیص است. اگرچه هیچ غذا یا رژیم غذایی خاصی وجود ندارد که کاملا بتواند از کولیت اولسراتیو و بیماری کرون پیشگیری و یا آنها را درمان کند، تغذیه و رژیم غذایی مناسب می تواند به بهبود علائم و کاهش التهاب روده کمک کند. نشان داده شده است که مصرف سبزیجات، میوه، آجیل، حبوبات، روغن زیتون و منابع پروتئینی بدون چربی مثل لوبیای سویا، گوشت مرغ و ماهی، اثر محافظتی در برابر ابتلا به IBD دارد و به بهبود جمعیت میکروبی روده کمک می کند. در مقابل، الگوهای غذایی غربی، سرشار از اسیدهای چرب غیراشباع امگا ۶، الکل، گوشت قرمز و افزودنیهای غذایی (نمک بیش از حد و شیرینکنندههای مصنوعی) التهاب روده را شدت بخشیده و میتوانند علائم این بیماری را بدتر کنند. به گفته محققین، رژیم غذایی غنی از اسیدهای چرب غیراشباع امگا ۶ (که معمولاً در روغنهای ذرت، سویا، گلرنگ و آفتابگردان یافت میشود) باعث التهاب روده میشود. در مقابل، رژیم غذایی غنی از روغن زیتون و حاوی اسیدهای چرب غیراشباع امگا ۳ (روغن ماهی) و چربی لبنیات باعث تقویت ایمنی در کولیت اولسراتیو می شود.
تغذیه درمانی در شرایط حاد بیماری
در شرایط حاد، بهترین رژیم درمانی ، تغذیه انترال (EEN) است که یک فرمولای مایع است. در این رژیم تمام مواد مغذی ضروری تامین می شود و هیچ غذای دیگری داده نمی شود. این رژیم بخصوص برای کاهش التهاب کودکان موثر است.. در نهایت، EEN باید برای مدت زمان محدودی استفاده شده و سپس غذا به تدریج اضافه می شود.
نتیجه گیری
امروزه رژیم غذایی مدیترانه ای برای افراد مبتلا به IBD که به دنبال یک رژیم غذایی متعادل و سالم هستند توصیه می شود.دانشمندان معتقدند تغذیه و نوع رژیم غذایی افراد IBD باید با توجه به شدت بیماری و آنچه در سبک زندگی آنها اتفاق می افتد، شخصی سازی شود. بنابراین مشاوره با یک متخصص تغذیه با تخصص در مدیریت IBD برای ایجاد یک برنامه فردی ضروری است. توصیه می کنیم قبل از انتخاب یکی از رژیمهای غذایی مد روز که بعضا بصورت آنلاین تبلیغ میشوند، با پزشک خود صحبت کنید تا شما را به یک متخصص تغذیه وارد در این بیماری معرفی کند و یک برنامه غذایی شخصیسازی شده برای شما تجویز شود.